The low-dose dexamethasone suppression test a reevaluation in patients with Cushing's syndrome
- 格式:pdf
- 大小:188.04 KB
- 文档页数:5

硕士学位论文论文题目粗聚焦高能震波在骨质疏松性骨折治疗中的作用研究生姓名黄海明指导教师姓名李晓林专业名称外科学研究方向骨关节创伤论文提交日期2013年5月粗聚焦高能震波在骨质疏松性骨折治疗中的作用中文摘要粗聚焦高能震波在骨质疏松性骨折治疗中的作用中文摘要骨质疏松症(osteoporosis,OP)是一种以骨量低下,骨微结构损坏,导致骨脆性增加,易发生骨折为特征的全身性骨病(世界卫生组织,WHO)。
随着全球人口老年化,骨质疏松性骨折发病率增加,其死亡率及致残率高,医疗费用巨大,已成为严重的公共健康问题。
骨质疏松性骨折愈合迟缓恢复期长,对骨质疏松性骨折患者不仅仅需要治疗现有的骨折,更重要的是要预防再次骨折的发生。
临床研究显示对骨质疏松性骨折患者进行治疗,可降低50%再骨折的发生。
但抗骨质疏松药物治疗抗骨质疏松药物治疗周期长,费用高,依从性差。
因此,探索防治骨质疏松症及其骨折的新途径十分必要。
高能震波(high energy shock waves, HESW )或体外冲击波(Extracorporeal Shock Wave)被证实有刺激骨痂生长,诱导血管再生,促进骨形成和镇痛等多种生物学效应,用于骨不连、股骨头坏死及骨肌系统慢性损伤疼痛等的治疗,是近来骨科领域的崭新非侵入性治疗方法。
粗聚焦高能震波由于焦点大治疗区域大,更适合骨科应用,本项目拟将粗聚焦高能震波应用于骨质疏松性骨折的治疗和再骨折的预防,以期望能促进骨愈合减少骨丢失,增加骨密度和骨强度;减轻疼痛使患者尽早恢复活动,减少并发症,防止再次骨折的发生。
本实验应用大鼠单纯去势法、兔双卵巢去势加肌注小剂量地塞米松的方法制作78只SD大鼠骨质疏松性骨折模型及24只新西兰大白兔骨质疏松模型方法。
造模成功后,应用粗聚焦高能震波仪Orthospec(TM)对准左侧检测区域,用能流密度0.26mj/mm2,频率60次/分,冲击量为2000次的高能震波治疗一次,右侧对照组不予治疗。
瞠凼坌鲨!芏塑苤查!!!!至!旦箜垫鲞箜!塑垦!i!』垦!!!型!!!塑!!坐!垒!g!塑!Q!!!!丛垫!盟!:!‘653・131例库欣综合征患者的临床特征分析周兴建杨国庆徐焱成李芳龚宇巴建明窦京涛母义明・肾上腺来源疾病・【提要】13l例(男性33例,女性98例)库欣综合征患者中,库欣病53例,肾上腺腺瘤49例,大结节增生12例,异位ACTH综合征16例,肾上腺皮质腺癌1例。
不同类型的库欣综合征患者在发病年龄、病程、8:00和0:00血皮质醇水平、24h尿游离皮质醇水平、空腹血糖、HbA.,、大剂量和小剂量地塞米松抑制后8:00皮质醇水平等指标有统计学差异(均P<0.05)。
16例异位AC‘l'I-I综合征患者来源于肺部5例,胰腺3例,胸腺2例,肝脏2例;来源不明4例。
131例库欣综合征患者中,合并糖尿病60例,糖耐量受损22例,血糖正常49例。
库欣综合征患者女性发病高于男性;不同类型的库欣综合征患者,主要临床表现及生化指标具有差异;糖代谢异常是库欣综合患者的常见临床表现,、【关键词】库欣综合征;临床特征Clinicalfeaturesof131patientswithCushingsyndromeZHOUXing-jian4,YANGGuo-qing,XUYan—cheng,L1Fang,GONGYu,BAJian—ruing,DOUring—tao,MUYi—ming.+DepartmentofEndocrinolog).ChinesePMGeneralHospital,Bering100853,ChinaCorrespondingauthor:MUK—ming,Email:mu)。
lining@301hospital.conl.cn【Summary】Onehundredandthirty—onepatientswithCushingsyndrome(33malesand98females)wereenrolled,including53easesofCushing’sdisease,49casesofadrenaladenoma,12casesofbignodularhyperplasia,16easeswithectopicAC‘rHsyndrome,and1casewithadrenalcoaicalcarcinoma.Theageofonset,duration,8:00and0:00plasmacortisollevels,24hurinaryfreecortisollevels,fastingplasmaglucose,HbAIc,8:00cortisollevelafterhigh・・andlow・・dosedexamethasonesuppressiontestweresignificantlydifferentamongdifferenttypesofCushingsyndrome(allP<0.05).Theprimarylesionin16casesofeetopicACTHsyndromewerefoundinlung(n=5),pancreas(n=3),thymus(n=2),liver(n=2),andunknownorigin(n=4).Therewere60casescombinedwithdiabetes(45.8%),22caseswithimpairedglucosetolerance(16.8%),and49caseswithnormaglycemia(37.4%)inthese131patients.TheprobabilityofCushingsyndromeinfemalewashigherthanthatinman.ThereweresignificantlydifferentfortheclinicalnmnifestationsandbiochemicalparametersamongdifferenttypesofCushingsyndrome.AbnormalglucosemetaholismisthecommonclinicalmanifestationsofpatientswithCushingsyndrome.【Keywords】Cushingsyndrome;Clinicalfeatures(ChinJEndocrinofMetab,2013,29:653-655)库欣综合征是机体长期、慢性的暴露于过多的糖皮质激素而引起的一种临床综合征。


库欣综合征专家共识(2011年)中华医学会内分泌学分会为规范库欣综合征的诊断和治疗,中华医学会内分泌学分会肾上腺学组参考2003年以来发表在JCEM上的共识、指南及meta分析,完成了专家共识的初稿后,联合垂体学组于2011年2月和4月分别召开两次学组会,进行充分讨论后修改定稿,并在2011年内分泌年会上解读,现予以公布。
库欣综合征的概况一、定义库欣综合征(Cushing7Ssyndrome,CS)又称皮质醇增多症,过去曾译为柯兴综合征,是由于多种病因引起肾上腺皮质长期分泌过量皮质醇所产生的一组症候群,也称为内源性库欣综合征;而长期应用外源性肾上腺糖皮质激素或饮用大量酒精饮料引起的类似库欣综合征的临床表现,称为外源性、药源性或类库欣综合征,本共识主要讨论内源性库欣综合征01-13]。
近年来将仅有实验室检查异常而无明显临床表现的类型称为亚临床库欣综合征。
二、发病率及死亡率欧洲数据显示库欣综合征的年发病率为2/100万人一3/100万人,男女比例约为1:3,国内尚缺乏大规模流行病学数据。
在某些特殊人群如2型糖尿病、骨质疏松和肾上腺意外瘤患者中,亚临床库欣综合征的比例较高。
库欣综合征患者的死亡率较正常人群高4倍,因其最重要和最常见的并发症为高血压、糖尿病、骨质疏松及代谢综合征,故增加了心血管疾病的危险性,导致库欣综合征患者的大多数死因为心、脑血管事件或严重感染。
但当高皮质醇血症缓解后,其标准化的死亡率(SMR)与年龄匹配的普通人群相当,若治疗后仍存在持续性中度皮质醇增多症的患者,与普通人群相比,SMR增加3.8-5倍。
三、库欣综合征的病因分类内源性库欣综合征分为ACTH依赖性和ACTH非依赖性,如表1所示。
库欣综合征的临床表现库欣综合征临床表现谱很广,常见的典型症状和体征见表2。
当临床表现典型时,库欣综合征易被诊断,但轻症患者的诊断则有一定难度。
少数症状和体征具有鉴别诊断意义,如新发皮肤紫纹、多血质、近端肌无力、非创伤性皮肤瘀斑和与年龄不相称的骨质疏松等;而库欣综合征儿童常伴有生长发育停滞;其他由皮质醇增多所致的肥胖、抑郁、糖尿病、高血压或月经不规律等也常见于普通人群中,因此,库欣综合征与非库欣综合征患者的临床表现有部分重叠。
18中国乡村医药杂志2008年6月第15卷第6期后循环缺血是指供应脑部的椎基底动脉缺血引起的病变,20%的缺血性脑血管病由后循环缺血引起的。
笔者采用奥扎格雷钠(丹奥)联合天麻素注射液治疗后循环缺血,疗效满意,现报道如下:1 临床资料1.1 一般资料及分组 选择我院自2004年2月至2006年5月住院治疗72例符合WHO后循环缺血诊断标准[1]。
排除标准:①颅内出血或蛛网膜下隙出血;②发作性位置性眩晕;③五官科疾病引起的眩晕;④颈椎病。
所有病例均经颅多普勒检查检测提示椎基底动脉狭窄或闭塞。
分为治疗组与对照组各36例。
两组均经颅内CT检查,其中治疗组提示后循环梗死9例(25.0%),对照组11例(30.6%);治疗组中15例(41.7%)行脑MRI检查发现梗死8例(8/15),对照组19例(52.8%)行MRI检查发现梗死10例(10/19)。
治疗组中男性16例,女性20例;年龄55~72岁,平均年龄(60.0±3.4)岁;病程8h~3d。
对照组男性18例,女性18例;年龄61~70岁,平均年龄(62.0±2.8)岁;病程10h至4d。
两组性别、年龄、病程等大体相似,有可比性。
1.2 治疗方法 治疗组采用丹奥(辽宁丹东制药厂生产)80mg加入0.9%氯化钠注射液250ml静脉滴注,一日一次,天麻素注射液600~800mg加入0.9%氯化钠注射液250ml静脉滴注,一日一次。
对照组予右旋糖酐500ml加复方丹参注射液20~30ml静脉滴注,一日一次。
两组均用拜阿司匹林及胞磷胆碱。
两组疗程均14天。
不用其他溶栓药物及活血化瘀中成药。
有颅内高压者行降颅压,有感染者行抗感染治疗。
1.3 疗效评定 参考相关文献[2-3]。
1.4 统计学处理 计量资料以x- ±s表示,采用t、χ2检验。
2 结果2.1 两组疗效及起效时间 见表1。
由表1可以看出,治疗组显效率、有效率、总有效率均高于对照组,但显效率、有效率差异无统计学意义,总有效率比较差异有统计学意义,治疗组疗效好于对照组。
小剂量地塞米松对新生儿胎粪吸入综合征患儿血清IL—5、IL—13和TNF—α的影响作者:黄上明袁毅肖万祥陈睿来源:《中国当代医药》2013年第18期[摘要] 目的探讨小剂量地塞米松对新生儿胎粪吸入综合征患儿血清中白介素-5(IL-5)、白介素-13(IL-13)和肿瘤坏死因子-α(TNF-α)的影响。
方法新生儿胎粪吸入综合征患儿40例,随机分为治疗组和对照组,除了治疗组从第1、2、3天加用小剂量地塞米松[0.5 mg/(kg·d)]治疗外,两组其余治疗方案均相同;以足月顺产的正常新生儿20例作为正常组。
检测3组研究对象第1、4、7天血清IL-5、IL-13、TNF-α的变化。
结果对照组第1、4、7天血清IL-5、IL-13、TNF-α水平均高于正常组(P < 0.05);对照组和治疗组第4天血清IL-5、IL-13、TNF-α明显升高,且对照组的水平高于治疗组(P < 0.05)。
结论在新生儿胎粪吸入综合征患儿治疗过程中,小剂量地塞米松可抑制炎症反应,减轻气道高反应性。
[关键词] 新生儿;胎粪吸入综合征;地塞米松;白细胞介素-5;白细胞介素-13;肿瘤坏死因子-α[中图分类号] R722 [文献标识码] A [文章编号] 1674-4721(2013)06(c)-0031-02Effect of the low-dose dexamethasone on the level of IL-5,IL-13,TNF-α in blood of newborn meconium aspiration syndromeHUANG Shangming YUAN Yi XIAO Wanxiang▲ CHEN Ru iShenzhen Baoan Maternal and Child Health Hospital,Guangdong Province,Shenzhen 518100,China[Abstract] Objective To investigate the effect of low-dose Dexamethasone on the level of IL-5,IL-13,TNF-α in blood of newborn meconium aspiration s yndrome. Methods 40 cases of neonatal meconium aspiration syndrome were randomly divided into treatment group and control group.Two groups were given the same treatment,except the treatment group from the three days of being hospitalized with a small dose Dexamethasone treatment.In addition,20 cases of normal neonates were taken as normal control group.The level of IL-5,IL-13,TNF-α in blood were determined at the first day,the fourth day,the seventh day,respectively. Results The level of IL-5,IL-13,TNF-α in control group were higher than in the normal control group (P < 0.05) at the first day,the fourth day,the seventh day.At the fourth day,the level of IL-5,IL-13,TNF-α in treatment group and control group increased obviously and were higher than in the normal control group (P < 0.05). Conclusion In neonates with meconium inhaled syndrome treatment process,dexamethasone can inhibit the inflammatory response and reduce airway high inflammatory reaction.[Key words] Newborn;Meconinum aspiration syndrome;Dexamethasone;Interleukin-5;Interleukin-13;Tumor necrosis factor-α胎粪吸入综合征(meconium aspiration syndrome,MAS)是新生儿常见的危重疾病之一。
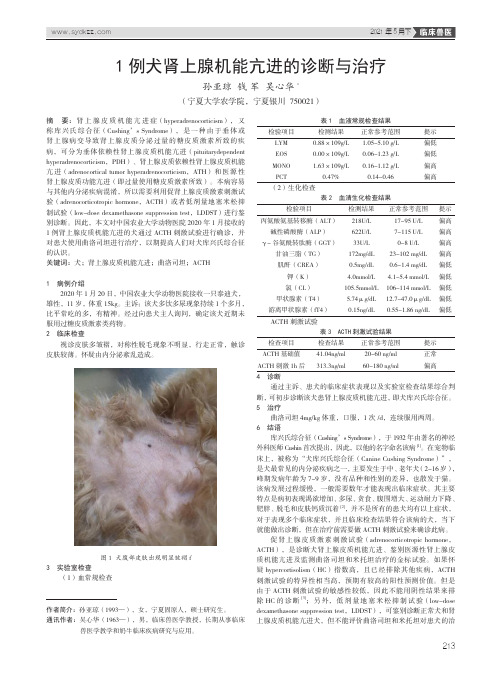
223低剂量地塞米松抑制试验诊断犬库兴氏综合征周永欢(天津市滨海新区塘沽动物疫病预防控制中心,天津 300450)摘 要:库兴氏综合征,即肾上腺皮质机能亢进,是由于体内糖皮质激素慢性过量分泌而引起的症候群。
最早为库兴医生发现,又称库兴氏综合征。
本试验应用低剂量地塞米松抑制试验来诊断犬的库兴氏综合征。
相比于促肾上腺皮质激素刺激试验,地塞米松抑制试验诊断准确,成本低,还可以用来分型,但诊断周期较长。
试验结果证明应用低剂量地塞米松抑制试验诊断犬库兴氏综合征是可行有效的。
关键词:犬库兴氏综合征;地塞米松;皮质醇在正常情况下,肾上腺皮质只有在促肾上腺皮质激素(ACTH)作用下才分泌皮质醇,当皮质醇超过生理水平时,ACTH 分泌就停止。
库兴氏综合征多是由于皮质醇或ACTH 分泌失控引起的:即肾上腺不受ACTH 作用能自行分泌皮质醇,或皮质醇对ACTH 分泌不能发挥正常的抑制作用。
肾上腺皮质机能亢进可分为垂体依赖性、肾上腺皮质依赖性和医源性(即由兽医或主人过量使用糖皮质激素所致)。
确诊肾上腺皮质机能亢进的试验包括ACTH 刺激试验、低剂量地塞米松抑制试验(low-dose dexamethasone suppression,LDDS)以及地塞米松抑制试验和ACTH 刺激试验结合试验(V 试验)。
本次试验通过试验犬和临床犬进行LDDS,分时段测犬血液中皮质醇浓度,得出各个时段的皮质醇含量,进行分析诊断。
1 材料1.1 试验动物试验犬3只,临床疑似病犬1只1.2 试验试剂地塞米松磷酸钠1.3 试验材料和仪器1ml 注射器,离心管,含可的松条形码标记试剂条,SPR 管,小型VIDAS 全自动化荧光酶标免疫测试系统,离心机。
2 方法2.1 试验犬低剂量地塞米松抑制试验(1)在给药前,早8:00先用注射器取试验犬血液1ml,血液静置20min,放入离心管进行离心,3500r/min,离心5min。
取血清100μl 到试剂条,放入小型VIDAS 全自动化荧光酶标免疫测试系统,进行皮质醇的测定。
库欣综合征本词条由好大夫在线特约专家提供专业内容并参与编辑窦京涛(主任医师)解放军总医院内分泌科库欣综合征(Cushing’s Syndrome,CS)又称皮质醇增多症(hvpercortisolism)或柯兴综合征,1921年美国神经外科医生Harvey Cushing 首先报告。
本征是由于多种病因引起肾上腺皮质长期分泌过量皮质醇所产生的一组症候群,主要表现为满月脸、多血质外貌、向心性肥胖、痤疮、紫纹、高血压、继发性糖尿病和骨质疏松等。
由于长期应用外源性肾上腺糖皮质激素或饮用大量含酒精饮料也可以引起类似库欣综合征的临床表现,且均表现为高皮质醇血症,故将器质性病变引起的称为内源性库欣综合征;外源性补充或酒精所致称为外源性、药源性或类库欣综合征。
目录1发病率及死亡率2临床表现3疾病检查4影像学检查5异位ACTH综合征病灶定位的特殊检查6特殊人群的检查7疾病治疗1发病率及死亡率丹麦的数据显示库欣综合征(CS)的年发病率为2/100万人;西班牙报告年发病率为2.5/100万人,患病率为39/100万人;美国密尔沃基地区调查结果为5/100万人;库欣综合征诊治指南年发病率平均为2~3/100万人。
本征可发生于任何年龄,成人多于儿童,女性多于男性,男女比例约为1:3~5。
国内尚缺乏大规模流行病学数据。
在某些特殊人群如2型糖尿病、高血压病、骨质疏松、多囊卵巢综合征、不孕/不育和肾上腺意外瘤患者中,亚临床库欣综合征的比例较高。
a满月脸 b水牛背 c腹部紫纹CS患者的死亡率较正常人群高4倍,因其最常见的并发症为高血压、糖尿病、骨质疏松及代谢综合征,这些并发症显著增加了心、脑血管疾病的危险性,导致CS患者的大多数死因为心、脑血管事件或严重感染。
上世纪早期严重高皮质醇血症患者的存活时间中位数为4.6年,1952年研究报告5年存活率为50%。
近年研究发现,当高皮质醇血症缓解后,其标准化的死亡率(SMR)与年龄匹配的普通人群相当,术后生活质量显著提高,但所有症状不一定完全缓解,随访15年发现,成功手术组生活质量较同年龄和同性别正常组比较降低;而治疗后仍存在持续性中度皮质醇增多症的患者,与普通人群相比,SMR增加3.8~5倍。
地塞米松提高多囊卵巢综合征排卵及妊娠率的分析摘要目的:探讨地塞米松联合促排卵药物对提高多囊卵巢综合征(PCOS)病人排卵率及妊娠率的效果。
方法:将52例PCOS患者随机分为观察组与对照组各26例。
观察组采用联合用药,在使用克罗米芬(CC)配合人绒毛膜促性腺激素(HCG)治疗的基础上,给予口服小剂量地塞米松;而对照组常规使用CC 和HCG。
观察比较两组排卵率及妊娠率情况。
结果:观察组在加用地塞米松后,排卵率较对照组有明显提高,差异有显著性(P<0.05)。
两组治疗后,妊娠率相比较差异无统计学意义(P>0.05)。
结论:联合使用地塞米松加促排卵药物在提高PCOS排卵率及妊娠数方面,比单用促排卵药物效果好。
关键词联合用药地塞米松PCOSPCOS是育龄妇女表现为多态性的内分泌及代谢异常性疾病,是女性无排卵性不孕的常见原因之一。
其发病率占育龄妇女5%~10%,占无排卵性不孕的50%~70%。
克罗米芬(CC)对PCOS无排卵的不孕患者,使其排卵率达80%,妊娠率达40%;但仍有一部分患者对克罗米芬无反应或卵泡未破裂黄素化。
有研究表明,糖皮质激素可有效降低PCOS患者的雄激素水平,改善CC的促排卵作用。
我科联合应用地塞米松治疗PCOS引起的不孕不育收到良好效果,现报告如下。
资料与方法一般资料:选择2008年10月~2010年9月我科就诊52例PCOS排卵障碍不孕患者,年龄23~38岁,平均28.3岁;不孕年限1~5年,平均3.5年。
原发不孕33例(63.5%),继发不孕19例(36.5%)。
平均体重指数在正常范围,且3个月内未使用过任何促排卵药物。
所有患者的骨密度、肝肾功能均正常,且无输卵管、子宫或其他内分泌异常及免疫学等不孕因素。
同时治疗前均征得患者知情同意。
方法:随机分为观察组与对照组各26例。
观察组于月经周期第1天开始口服地塞米松0.75mg,直至排卵停药;月经周期第5天开始口服CC 50~100mg,共5天;月经周期第8天口服补佳乐2mg,至排卵或内膜达1cm停药;月经周期第11天开始B超监测卵泡发育情况,卵泡直径≥18~20mm时,肌注HCG 1万U。

•38•Chinese Practical Journal of Rural Doctor 2021 Vol.28 No.l论著低剂量地塞米松减轻全膝关节置换术后疼痛和恶心呕吐疗效的荟萃分析兔卓_________作荇单位:11〇〇3丨沈阳,沈阳市第四人民医院麻醉科【摘要】目的对地塞米松在全膝关节置换术镇痛和降低恶心呕吐发生率中的疗效进行评估。
方法在中英文数据库中检索2005年7月10丨J 2020年7月10日期间发表的地塞米松在全膝关节置换术中的应用相关研究文献,使用Review Manager 5.3对文献中相关数据进行统计分析。
结果共有11项研究纳入研究,meta分析显示,地塞米松组与对照组视觉模拟疼痛评分在术后12 h、48 h、72 h及总效应上差异有统I卜学意义(PC0.05);两组术后6 h视觉模拟疼痛评分差异无统计学意义(P〉0.05>。
地塞米松组与对照组在术后恶心发生率、呕吐发生率、止吐药需求率及炎症指标水平上差异有统计学意义(P<〇.〇5);地塞米松组与对照组术后住院时间差异无统计学意义(P>0.05)。
结论Meta分析表明,地塞米松虽然不能缩短全膝关节置换术患者的住院时间,但可以有效降低术后疼痛程度、炎症指标水平、恶心呕吐发生率和止吐药需求率,这对患者术后的快速恢复具有重要意义。
【关键词】全膝关节置换术;地塞米松;疼痛;恶心:呕吐;荟萃分析【中图分类号】R614【文献标识码】八【文章编号】1672-7185(2021)01 -0038-06 doi: 10.3969/j.issn. 1672-7185.2021.01.014Efficacy of Low-Dose Dexamethasone in Reducing Pain, Nausea and Vomiting after Total Knee Arthroplasty: A Meta-AnalysisL I Zhuo(Department of Anesthesiology. The 4th People's Hospital of Shenyang, Shenyang 110031, Liaoning Province, China)【Abstract】Objective To evaluate the effect of dexamethasone on analgesia, nausea and vomiting in total knee arthroplasty. Methods The literatures on the application of dexamethasone in total knee arthroplasty published from July 10th, 2005 to July 10th, 2020 were searched in Chinese and English databases, and the relevant data in the literatures were statistically analyzed by Review Manager 5.3. Results A total of 11studies were included in the study. Meta-analysis showed that there were significant differences in visual analog pain scores between dexamethasone group and control group at 12 hours, 48 hours, 72 hours after operation and total effect (P < 0.05); there was no significant difference in visual analog pain score between the two groups at 6 hours after operation {P > 0.05). There were significant differences between dexamethasone group and control group in the incidence of postoperative nausea, vomiting, antiemctic drug demand rate and inflammatory index level (P < 0.05). There was no significant difference in postoperative hospital stay between dexamethasone group and control group (P >0.05). Conclusion Mcta-analysis showed that dexamethasone could not shorten the hospitalization time of patients undergoing total knee arthroplasty, but it could effectively reduce the degree of postoperative pain, the level of inflammatory indicators, the incidence of nausea and vomiting and the demand rate of antiemetic drugs, which is of g reat significance for the rapid recovery of patients after surgery.【Key Words】Total Knee Arthroplasty; Dexamethasone; Pain; Nausea; Vomiting; A Meta-Analysis全膝关节置换术(TK A>是治疗晚期膝关节 美国在2015年大约完成70万台TKA手术w。
[收稿日期]2023-01-30 [修回日期]2023-12-30[基金项目]安徽省淮南市科技计划项目(2020091)[作者简介]刘明红(1981-),女,硕士研究生导师,副主任医师.[文章编号]1000⁃2200(2024)03⁃0344⁃04㊃临床医学㊃小剂量地塞米松复合罗哌卡因行舌咽神经阻滞对小儿全麻术后疼痛及炎症反应的影响刘明红,李 菊,陈慧春,石 军(安徽理工大学第一附属医院麻醉科,232000)[摘要]目的:观察小剂量地塞米松复合盐酸罗哌卡因行舌咽神经阻滞对小儿扁桃体切除术后疼痛及炎症反应的影响㊂方法:选择行小儿扁桃体切除术的择期患儿80例,ASA 分级Ⅰ~Ⅱ级㊂采用随机数字法分为2组,罗哌卡因组(L 组)和复合组(LD 组),各40例㊂L 组采用0.25%盐酸罗哌卡因共2mL,LD 组采用0.25%盐酸罗哌卡因+地塞米松0.1mg /kg 共2mL㊂记录术后即刻㊁术后24h㊁2组术后48h 患儿静息及吞咽时FLACC 评分㊁炎症因子水平及不良反应发生率等㊂结果:术后48h LD 组的FLACC 评分比L 组低(P <0.05);LD 组术后首次进食时间比L 组更早(P <0.01);LD 组术后即刻和48h C 反应蛋白(CRP)㊁白细胞介素(IL)⁃1β㊁IL⁃6水平均比L 组低(P <0.05);LD 组术后发热发生率低于L 组(P <0.05)㊂结论:小剂量地塞米松复合罗哌卡因进行舌咽神经阻滞,可明显降低小儿扁桃体切除术后的疼痛,减少术后发热的发生,减轻术后炎症反应,为小儿扁桃体切除术提供了一种有效的超前镇痛方法㊂[关键词]舌咽神经阻滞;术后镇痛;炎症反应;儿童[中图法分类号]R 614 [文献标志码]A DOI :10.13898/ki.issn.1000⁃2200.2024.03.014Effect of the glossopharyngeal nerve block of low dose dexamethasone combined with ropivacaine on postoperative pain and inflammation in children after general anesthesiaLIU Minghong,LI Ju,CHEN Huichun,SHI Jun(Department of Anesthesiology ,The First Affiliated Hospital of Anhui University of Science and Technology ,Huainan Anhui 232000,China )[Abstract ]Objective :To observe the glossopharyngeal nerve block of low dose dexamethasone combined with ropivacaine hydrochloride on pain and inflammation in children after tonsillectomy.Methods :Eighty children with ASA grade Ⅰ-Ⅱscheduled by pediatric tonsillectomy were randomly divided into two groups(40cases in each group):ropivacaine group(Group L)and combination group(LD Group LD).The Group L was given 0.25%ropivacaine hydrochloride (2mL),and the Group LD was given 0.25%ropivacaine hydrochloride combined with dexamethasone 0.1mg /kg(2mL).The FLACC scores,levels of inflammatory factors and incidence of adverse reactions at rest and during swallowing were recorded immediately after surgery,after 24h and 48h of surgery in two groups.Results :The FLACC score in the Group LD was lower than that in L group at 48h after operation(P <0.05).The first feeding time of Group LD was earlier than that of Group L(P <0.01).The levels of C⁃reactive protein(CRP),interleukin(IL)⁃1βand IL⁃6immediately and at 48h after surgery in the Group LD were lower than those in Group L (P <0.05).The incidence of postoperative fever in the Group LD was lower than that in Group L (P <0.05).Conclusions :The glossopharyngeal nerve block of low dose dexamethasone combined with ropivacaine hydrochloride can obviously reduce the pain after tonsillectomy in children,occurrenceof postoperative fever and postoperative inflammation,and provide an effective pre⁃analgesic method for children tonsillectomy.[Key words ]glossopharyngeal nerve block;postoperative analgesia;inflammatory response;children 小儿扁桃体切除术是耳鼻喉科的常见手术,数量多占比重,但存在拔管时呛咳㊁术后咽痛㊁术后发热㊁吞咽困难等不良反应,严重者甚引起患儿恐惧和焦虑心理,不利术后康复[1]㊂而且患儿多为低龄儿童,存在表达困难㊂因此,术后疼痛常被忽视㊂目前儿童扁桃体切除术后的镇痛方案多以阿片类药物静脉镇痛为主,但不良反应多㊂因此,寻找合适的镇痛方法既可减轻患儿术后疼痛,又可减少不良反应,显得尤为重要㊂纵观文献发现:舌咽神经阻滞可以有效减轻儿童扁桃体切除术后的早期疼痛[2]㊂本研究旨在通过前瞻性随机对照研究,探讨小剂量地塞米松复合罗哌卡因进行舌咽神经阻滞术后镇痛时间㊁镇痛效果及不良反应㊂现作报道㊂1 资料与方法1.1 研究对象 本研究已获得医院医学伦理委员会审核批准(2021-伦审-030)选取2021-2022年在我院行扁桃体切除术的患儿80例㊂所有患儿监护人均同意并签署知情同意书㊂年龄3-13岁,体质量指数(BMI)(31.45±11.00)kg/m2㊂纳入标准:(1)年龄3~13岁;(2)美国麻醉师协会(ASA)分级为Ⅰ~Ⅱ级;(3)择期行扁桃体切除术的住院患儿;(4)手术时间应在120min以内;(5)自愿参加并签署知情同意书㊂排除标准:(1)患有精神疾病;(2)严重沟通表达障碍;(3)BMI>45kg/m2;(4)术前24h使用了镇静或镇痛药物;(5)2个月内参加过其他药物试验㊂剔除标准:(1)病人撤回知情同意书;(2)不符合入组标准或符合排除标准的病人;(3)失访㊂剔除病例不作疗效统计分析㊂1.2 分组方法 采用随机数字法分为2组,罗哌卡因组(L组)和复合组(LD组),各40例㊂L组采用0.25%盐酸罗哌卡因2mL,LD组采用0.25%盐酸罗哌卡因2mL+地塞米松0.1mg/kg㊂2组患儿在年龄㊁体质量㊁出血量㊁手术时长㊁麻醉时长等基本资料差异均无统计学意义(P>0.05)(见表1)㊂1.3 方法 所有患儿术前常规禁食8h㊁禁饮2h㊂入手术室后开放上肢外周静脉通道,按5mL㊃kg-1㊃h-1的速率输注乳酸林格液[12]㊂鼻导管吸氧3L/min (预吸氧3min后开始麻醉),进行无创血压(NIBP)㊁6导联心电图(ECG)㊁血氧饱和度(SpO2)和麻醉深度(BIS)监测,记录基础值㊂选用静脉麻醉,术前用药,甲泼尼龙0.5mg/kg+阿托品0.005mg/kg㊂静脉诱导,阿芬太尼0.5μg/kg,丙泊酚2.5mg/kg,顺式阿曲库胺0.01mg/kg㊂术中使用丙泊酚和瑞芬太尼持续静脉泵注,维持BIS值在40~60之间,根据顺式阿曲库代谢时间追加用药㊂在患儿双侧扁桃体摘除后,进行双侧舌咽神经阻滞㊂由同一麻醉医师进行舌咽神经阻滞(扁桃体支),即咽腭皱襞(后扁桃体支柱)的中点,针头刺破咽后壁黏膜,将其插入咽壁,深度约0.5cm㊂经过仔细回抽,无血无气后,罗哌卡因组(L组)缓慢注射0.25%盐酸罗哌卡因共2mL;复合组(LD组)缓慢注射0.25%盐酸罗哌卡因2mL+地塞米松0.1mg/kg;待患儿呼吸恢复且规律,脱氧5min,SpO2持续>95%后,拔除气管导管,送回PACU观察30min㊂1.4 评价指标 (1)疼痛评价:静息及吞咽时在术后即刻(T1)㊁术后24h(T2)㊁术后48h(T3)采用FLACC量表[3],对患儿面部表情㊁腿部姿势㊁躯体活动度㊁哭闹㊁是否安慰进行评分㊂评估总分:0分=放松㊁舒适;1~3分=轻微不适;4~6分=中度疼痛;7~10分=严重疼痛㊁不适㊂(2)患儿恢复时间包括:拔管时间指从停全麻药到拔除气管导管的时间;手术时间;术毕到首次进食流质食物时间㊂(3)C反应蛋白(CRP)㊁白细胞介素(IL)⁃1β㊁IL⁃6水平:分别抽取患儿术前(T0)㊁术后即刻(T1)㊁术后48h(T3)静脉血3mL离心处理后,采用酶联免疫吸附试验(ELISA)检测㊂(4)术后不良反应:拔管时呛咳㊁恶心呕吐㊁术后发热㊁局麻药中毒㊁呼吸困难㊁心律失常等不良反应的发生率㊂1.5 统计学方法 采用t(或t′)检验和χ2检验㊂2 结果2.1 2组一般资料比较 2组患儿年龄㊁体质量㊁出血量㊁手术时长㊁麻醉时长比较,差异均无统计学意义(P>0.05)(见表1)㊂表1 2组一般资料比较(x±s)分组n年龄/岁体质量/(kg/m2)出血量/mL手术时长/min麻醉时长/min L组40 6.15±2.7131.61±10.534.77±1.9240.25±13.3950.62±8.33 LD组40 6.27±2.6331.30±11.484.47±2.1039.75±13.1051.12±9.02 t 0.200.160.670.170.26P >0.05>0.05>0.05>0.05>0.05 2.2 2组FLACC评分比较 2组患儿在术后即刻(T1)㊁术后24h(T2)静息及吞咽时的FLACC评分差异均无统计学意义(P> 0.05)㊂术后48h(T3)LD组的患儿静息及吞咽时FLACC评分均低于L组(P<0.05)(见表2)㊂2.3 2组患儿恢复时间比较 与L组相比,LD组术后首次进食时间更短(P<0.01);2组手术时间和拔管时间差异均无统计学意义(P>0.05)(见表3)㊂2.4 2组CRP㊁IL⁃1β㊁IL⁃6水平比较 术前2组患儿的CRP㊁IL⁃1β㊁IL⁃6比较,差异无统计学意义(P>0.05)㊂与L组相比,LD组在T1㊁T3时间点的CRP㊁IL⁃1β㊁IL⁃6水平均较低(P<0.05)(见表4)㊂表2 2组不同时间点FLACC评分比较(x±s;分)分组n静息时 T1 T2 T3 吞咽时 T1 T2 T3 L组40 4.25±0.74 3.85±0.62 3.17±0.75 4.76±0.78 4.04±0.58 3.45±0.69 LD组40 4.17±0.87 3.80±0.79 2.78±0.73 4.65±0.84 3.93±0.47 3.11±0.77 t 0.440.31 2.360.610.93 2.08P >0.05>0.05<0.05>0.05>0.05<0.05表3 2组患儿恢复时间比较(x±s)分组n 首次进食时间/h手术时间/min拔管时间/minL组408.52±2.4440.25±13.39 5.99±4.01 LD组40 6.07±3.1839.75±13.10 6.01±3.05t 3.870.170.03P <0.01>0.05>0.05 2.5 2组不良反应比较 2组拔管时呛咳㊁恶心呕吐发生率差异无统计意义(P>0.05),LD组术后发热发生率低于L组(P<0.05)(见表5);2组患儿术后均未出现呼吸困难㊁麻药中毒及心律失常的不良反应㊂3 讨论 临床上患儿在行双侧扁桃体切除术后,常发生拔管呛咳㊁发热㊁严重的咽部疼痛㊁异物感等㊂现正处于后疫情时代,若拔管时发生呛咳会导致呼吸道的气溶胶播散,可致病毒再次传播㊂若术后出现发热症状,则易与新冠感染症状相混淆㊂影响患儿在这一特殊时期的快速康复㊂另外,术后严重的咽部疼痛,会导致患儿烦躁不安㊁哭闹不止㊁不愿进食等,严重影响患儿身心健康[4]㊂表4 2组CRP㊁IL⁃1β㊁IL⁃6比较(x±s)分组nCRP/(mg/L) T0 T1 T3 IL⁃1β/(ng/L) T0 T1 T3 IL⁃6/(ng/mL) T0 T1 T3 L组40 3.25±1.0119.07±4.1417.55±3.4536.75±1.6340.85±1.4438.83±3.088.42±0.8120.68±1.8513.35±1.08 LD组40 3.30±0.9817.10±2.7615.43±5.3736.60±2.0539.90±2.1337.38±3.278.40±0.9019.82±1.3812.90±0.82 t 0.22 2.50* 2.10*0.36 2.34* 2.040.10 2.36 2.10 P >0.05<0.05<0.05>0.05<0.05<0.05>0.05<0.05<0.05 *示t′值表5 2组不良反应比较[n;百分率(%)]分组n拔管呛咳恶心呕吐术后发热L组403(7.5)3(7.5)8(20.0) LD组402(5.0)1(2.5)2(5.0)χ2 0.010.26 4.11P >0.05>0.05<0.05 从解剖学上看,扁桃体是由咽丛㊁上颌神经的腭后神经以及舌咽神经扁桃体支等神经共同所支配,而舌咽神经是支配扁桃体感觉的主要神经[5]㊂当扁桃体被切除后,舌咽神经可被充分暴露,而且其位置相对固定㊂可在扁桃体外侧筋膜间隙轻松找到舌咽神经[6]㊂文献[7]报道,切除扁桃体后,也可见舌咽神经横跨扁桃体窝内㊂因此,舌咽神经被完善的阻滞后,可以明显缓解患儿术后的咽部疼痛,这一观点已被文献证实㊂在前期预实验中发现:由于低龄患儿的扁桃体窝较小,当单侧注射5mL容量的局麻药时,扁桃体窝会出现明显肿胀,使其咽部空间变窄,存在拔管后患儿呼吸不畅的隐患㊂因此,本次实验中采用每侧小剂量(1mL)盐酸罗哌卡因进行舌咽神经阻滞的方案,也可以达到完善的舌咽神经阻滞㊂实验结果发现:良好的咽部镇痛,可以降低拔管时呛咳的发生率,减少病毒传播的风险;添加了佐剂地塞米松后,患儿术后48h的疼痛评分明显低于其他2组,说明复合佐剂地塞米松延长了舌咽神经阻滞的镇痛时间和镇痛效果㊂与以前文献报道的加入了佐剂地塞米松可以延长神经阻滞时间的结论相一致[8-9]㊂本研究是采用咽腭襞入路进行舌咽神经阻滞[10],其优势是更接近舌咽神经的发出部位,使用小容量局麻药就能够完善阻滞舌咽神经的感觉纤维,而且操作方便㊂术后随访时发现:患儿在切除肥大的扁桃体后,常出现术后发热症状,体温在37.3~38.6℃㊂究其可能的原因,一是扁桃体切除后,通常会有细菌释放入血的过程,会出现生理性发热,一般体温不超过38℃;二是伤口发生细菌感染或病毒感染,导致机体发生炎症反应[11]㊂而在临床检验中,C反应蛋白是监测术后感染程度的重要指标,可以快速反应机体炎症变化,是人体急性时相反应最主要的敏感标志物之一[12]㊂CRP是炎性淋巴因子,如:IL⁃6㊁IL⁃1㊁肿瘤坏死因子等,刺激肝脏和上皮细胞合成[13]㊂本研究结果显示,各组患儿术后的炎症因子CRP㊁IL⁃1β㊁IL⁃6呈现先升后降的趋势㊂给予神经阻滞后,患儿的炎症因子水平明显降低,加入佐剂地塞米松后炎症因子水平更低㊂这与复合地塞米松的神经阻滞组患儿术后发热明显减少的结果相一致,可能与地塞米松减少炎症因子的释放,增强术后机体抗感染的能力有关㊂众所周知,地塞米松可以降低炎症因子在局部的聚集[14],降低机体炎症反应,预防术后感染的发生[15-16]㊂所有患儿均未出现局麻药中毒㊁呼吸困难及心律失常这些不良反应,舌咽神经阻滞并未给患儿带来明显的不利影响㊂而且,复合地塞米松的患儿术后恶心呕吐的发生率明显降低,可能与地塞米松作为神经阻滞的佐剂有关㊂文献[17]报道,地塞米松的止吐作用与它的免疫抑制作用有关㊂临床上经常使用地塞米松治疗多种癌症药物化疗引起的急性和延迟恶心和呕吐[18-19]㊂综上所述,小剂量地塞米松复合罗哌卡因用于舌咽神经阻滞,作为小儿扁桃体切除术后的一种镇痛方法,具有镇痛效果好㊁炎症反应轻㊁舒适度高的优点㊂该方法还可以明显减少拔管后呛咳㊁术后发热㊁恶心呕吐的不良反应,在后疫情这一特殊时期,值得推广㊂[参考文献][1] HAN CL,RONG FU,LEI WF.Beneficial effects ofdexmedetomidine on early postoperative cognitive dysfunction inpediatric patients with tonsillectomy[J].Exp Ther Med,2018,16(1):420.[2] HEE⁃PYOUNG P,JUNG⁃WON H,SANG⁃HYUN P,et al.Theeffects of glossopharyngeal nerve block on postoperative pain reliefafter tonsillectomy:the importance of the extent of obtunded gagreflex as clinical indicator[J].Anesth Analg,2007,105(1):267.[3] REDMANN AJ,WANG Y,FURSTEIN J,et al.The use of theFLACC pain scale in pediatric patients undergoingadenotonsillectomy[J].Int J Pediatric Otorhinolaryngol,2017,92:115.[4] SAKKI AJ,MÄKINEN LK,KANERVA M,et al.Monopolartonsillotomy versus cold dissection tonsillectomy in children:Prospective study on postoperative recovery[J].Int J PediatricOtorhinolaryngol,2021,141:110513.[5] 康尧杰,覃爱玲.舌咽神经阻滞对儿童扁桃体切除术后疼痛的影响[J].中国耳鼻喉颅底外科杂志,2020,26(6):698. [6] AHMED SA,OMARA AF.The effects of glossopharyngeal nerveblock on post⁃tonsillectomy pain of children;randomizedcontrolled trial[J].Anesth Pain Med,2019,9(2):e90854. [7] 闫智强,张新海,尹兴红.儿童扁桃体切除术中舌咽神经舌支的裸露及临床意义[J].中华解剖与临床杂志,2021,26(5):589.[8] 盛芳,李男,谭文斐,等.右美托咪定或地塞米松复合罗哌卡因对椎旁神经阻滞效果的影响[J].临床麻醉学杂志,2021,37(2):150.[9] 戴鹏,王汉兵,刘洪珍,等.超声引导下罗哌卡因复合地塞米松腰方肌阻滞对全髋关节置换术患者术后镇痛的影响[J].临床麻醉学杂志,2021,37(11):1134.[10] SINGH N,SINGH S,MISHRA NK,et parison of extraoraland intraoral routes of glossopharyngeal nerve block for pain reliefin patient with carcinoma tongue:a prospective randomized study[J].J Cancer Res Ther,2020,16(3):534.[11] MITCHELL RB,ARCHER SM,ISHMAN SL,et al.Clinicalpractice guideline:tonsillectomy in children(update)[J].Otolaryngol Head Neck Surg,2019,160(1):1. [12] PLAT VD,VOETEN DM,DAAMS F,et al.C⁃reactive proteinafter major abdominal surgery in daily practice[J].Surgery,2021,170(4):1131.[13] WINSEN MV,MCSORLEY ST,MCLEOD R,et al.PostoperativeC⁃reactive protein concentrations to predict infective complicationsfollowing gastrectomy for cancer[J].J Surg Oncol,2021,124(7):1060.[14] KANEGUCHI A,OZAWA J,YAMAOKA K.Anti⁃inflammatorydurg dexamethasone treatment during the remobilization periodimproves range of motion in a rat knee model of joint contracture[J].Inflammation,2018,41(4):1409.[15] JACKSON KJ,AKROBETU D,GUDURU A,et al.Intracanaliculardexamethasone insert or topical prednisolone following istent andhydrus surgery for glaucoma[J].J Glaucoma,2022,31(8):694.[16] 蒋世杰,王禹基,赵公吟,等.小剂量地塞米松对老年前路全款关节置换术后疼痛及炎症反应的影响[J].中国老年学杂志,2020,40(15):3240.[17] CHEN WENJIE,LI GP,JIANG KE.Dexamethasone forpostoperative nausea and vomiting in papillary thyroid carcinomapatienta:a randomized clinical trial[J].J Am Coll Surg,2022,235(3):454.[18] SUH KJ,YOON S,KIM JW,et al.A single⁃arm feasibility studyof gradual dose de⁃escalation of antiemetic dexamethasone forolder patients receiving chemotherapy[J].J Geriatric Oncol,2021,12(6):922.[19] HATANO K,FUJIWARA SI,UMINO K,et al.Clinical interactionbetween dexamethasone and aprepitant in chemotherapy forlymphoma[J].Annal Hematol,2022,101:1211.(本文编辑 刘畅)。
过夜地塞米松抑制试验流程The overnight dexamethasone suppression test (DST) is a diagnostic procedure used to assess the functioning of the hypothalamic-pituitary-adrenal (HPA) axis. This test is primarily used in the evaluation of Cushing's syndrome, a condition characterized by excessive cortisol production. The DST involves the administration of dexamethasone, a synthetic glucocorticoid, and the subsequent measurement of cortisol levels. In this response, we will discuss the procedure, its significance, potential complications, and patient experience.The overnight DST begins with the administration of a low dose of dexamethasone, typically 1 mg, orally at 11 pm. The patient is instructed to fast overnight and return to the healthcare facility the following morning. Blood samples are then collected at 8 am to measure cortisol levels. In a normal individual, the administration of dexamethasone would suppress cortisol production, resulting in low cortisol levels. However, in patients with Cushing'ssyndrome, cortisol levels remain elevated despite the administration of dexamethasone.This test is crucial in the diagnosis of Cushing's syndrome as it helps differentiate between two types: ACTH-dependent and ACTH-independent. ACTH-dependent Cushing's syndrome is characterized by excessive production of ACTH,a hormone that stimulates cortisol production. In this case, the DST would result in cortisol suppression. On the other hand, ACTH-independent Cushing's syndrome is caused by adrenal tumors that produce cortisol independently of ACTH stimulation. In this case, cortisol levels would not be suppressed by the DST.While the overnight DST is a relatively safe procedure, there are potential complications that need to be considered. Dexamethasone is a potent glucocorticoid andcan cause side effects such as fluid retention, increased blood pressure, and glucose intolerance. These side effects are usually temporary and resolve once the medication is discontinued. However, it is essential to monitor patients closely for any adverse reactions during the test.From a patient's perspective, undergoing the overnight DST can be an anxiety-inducing experience. The need to fast overnight and the anticipation of blood collection can cause stress and discomfort. It is crucial for healthcare providers to provide clear instructions and address any concerns or fears the patient may have. Creating a calm and supportive environment can help alleviate some of the patient's anxiety and improve their overall experience.Furthermore, it is essential to consider the emotional impact of the test results on the patient. A positiveresult indicating cortisol suppression can provide relief for patients who have been experiencing symptoms of Cushing's syndrome. It can validate their concerns and provide a starting point for further investigation and treatment. Conversely, a negative result can be disheartening for patients who have been hoping for a definitive diagnosis. In such cases, it is crucial for healthcare providers to offer support and explain the next steps in the diagnostic process.In conclusion, the overnight dexamethasone suppression test is a valuable diagnostic tool in the evaluation of Cushing's syndrome. It helps differentiate between ACTH-dependent and ACTH-independent forms of the condition and guides further investigation and treatment. While the procedure itself is relatively safe, it is important to monitor patients for potential complications. Additionally, healthcare providers should be mindful of the emotional impact the test and its results can have on patients and provide appropriate support and guidance throughout the process.。

小剂量地塞米松治疗急性高血压脑岀血患者术后顽固性脑水肿的临床分析彭敏,段继新,于汉昌,王承(湖南省长沙市中医医院〔长沙市第八医院〕神经外科,湖南长沙410100)揖摘要】目的探讨小剂量地塞米松治疗急性高血压脑岀血患者术后顽固性脑水肿的临床效果。
方法选择2018年10月耀2019年10月收治的急性高血压脑岀血术后顽固性脑水肿患者60例,依据随机数字表分为观察组(n=30)及对照组(n=30)。
对照组行大剂量地塞米松治疗;观察组术后第3天开始加用小剂量地塞米松治疗。
比较两组手术前后脑水肿面积、美国国立卫生研究院卒中量表(NIHSS)评分、格拉斯哥昏迷量表(GCS)评分。
结果术后4d、6d、9d、12d,两组脑水肿面积均大于术前,差异有统计学意义(P<0.05);但手术后两组水肿面积随时间延长而减小,且观察组均小于对照组,差异有统计学意义(P<0.01)遥术前两组NIHSS评分、GCS评分组间比较,差异均无统计学意义(P>0.05);手术后2周,两组NIHSS评分低于术前,且观察组低于对照组,两组GCS评分明显高于术前,且观察组高于对照组,差异有统计学意义(P<0.01)遥结论小剂量地塞米松治疗急性脑岀血术后顽固性脑水肿可有效减小脑水肿面积,促进患者神经功能恢复,改善患者意识状态。
揖关键词】急性高血压脑岀血;顽固性脑水肿;地塞米松中图分类号:R651.1+9文献标志码:A DOI:10.3969/j.issn.1003-1383.2021.03.010Clinical analysis of low dose dexamethasone in the treatment of postoperative intractable cerebral edema in patients with acute hypertensive intracerebral hemorrhagePENG Min,DUAN Jixin,YU Hanchang,WANG Cheng(Department of Neurosurgery,Changsha Hospital of Traditional Chinese Medicine—Changsha Eighth Hospital,Changsha410100,Hunan,China)揖Abstract]Objective To investigate the clinical effect of low-dose dexamethasone in the treatment of postoperative intractable cerebral edema in patients with acute hypertensive intracerebral hemorrhage.Methods60patients with postoperative intractable cerebral edema after operation of acute hypertensive cerebral hemorrhage who admitted to hospital from October2018to October2019were selected and randomly divided into observation group(n=30)and control group(n=30).The control group were treated with high dose dexamethasone,and the observation group were treated with low dose dexamethasone from the third day after operation.And then,brain edema area,the National Institutes of Health Stroke Scale(NIH-SS)score and Glasgow Coma Scale(GCS)score before and after operation were compared between the two groups.Results 4d,6d,9d and12d after operation,the areas of brain edema in the two groups were larger than those before operation,and difference was statistically significant(P<0.05).After operation,however,the edema areas of the two groups decreased with time,and that of the observation group was smaller than that of the control group,and difference was statistically significant(P<0.01).There were no statistically significant differences in NIHSS scores and GCS scores between the two groups before operation(P>0.05).2weeks after operation,NIHSS scores of the two groups were lower than those before operation,and that of the observation group was lower than that of the control group,GCS scores of the two groups were significantly higher than those before operation,and that of the observation group was higher than that of the control group,and difference was statistically significant(P<0.01).Conclusion Low dose dexamethasone in the treatment of postoperative作者简介:彭敏,男,主治医师,医学硕士,研究方向:脑外伤。
化脓性扁桃体炎多由A组β链球菌感染所诱发的腭扁桃体急性化脓性炎症[1-2],是一种在临床上很常见的上呼吸道感染性疾病,儿童与青少年为高发人群[3-4]。
临床上多表现为明显咽痛,畏寒,高热,发病急,易反复等[5-6]。
因而对于化脓性扁桃体炎的治疗可采取对应抗生素治疗作为主要的手段[7],迄今为止,A组β链球菌对青霉素仍敏感。
该次研究采取该院在2016年1月—2018年1月期间接受治疗的小儿化脓性扁桃体炎患儿80例作为研究对象进行研究,现报道如下。
1资料与方法1.1一般资料随机选择在该院接受治疗的小儿化脓性扁桃体炎DOI:10.16662/ki.1674-0742.2018.27.124阿莫西林/克拉维酸钾联合短期地塞米松治疗小儿化脓性扁桃体炎的疗效观察王莉江苏省如皋市第三人民医院儿科,江苏如皋226531[摘要]目的探究阿莫西林/克拉维酸钾联合短期小剂量地塞米松治疗小儿化脓性扁桃体炎的疗效和安全性。
方法随机选取该院在2016年1月—2018年1月期间接受治疗的小儿化脓性扁桃体炎患儿80例作为研究对象进行研究,随机分为对照组和观察组患儿各40例,其中对照组单纯使用阿莫西林克拉维酸钾静脉滴注抗感染及对症支持治疗,观察组在对照组的基础上短期使用小剂量地塞米松进行治疗,对比两组患儿的临床疗效以及用药安全性。
结果观察组患儿的一般情况改善时间为(2.12±0.18)d,脓苔消失时间为(2.02±0.8)d,退热时间为(2.07±0.59)d,均显著低于对照组(t=5.273、4.386、4.012,P<0.05);观察组患儿治疗总有效率为97.50%,显著高于对照组患儿(χ2=18.131,P<0.05);两组患儿均未有不良反应出现。
结论采取阿莫西林克拉维酸钾的基础上短期使用小剂量地塞米松进行治疗小儿化脓性扁桃体炎,具有更显著的治疗效果,安全性高,值得临床参考。
[关键词]阿莫西林/克拉维酸钾;地塞米松;小儿化脓性扁桃体炎;效果;安全性[中图分类号]R725[文献标识码]A[文章编号]1674-0742(2018)09(c)-0124-03 Therapeutic Effect of Amoxicillin/Clavulanate Potassium Combined with Short-term Dexamethasone on Children with Suppurative TonsillitisW ANG LiDepartment of Pediatrics,Third People's Hospital of Rugao,Rugao,Jiangsu Province,226531China[Abstract]Objective To investigate the efficacy and safety of amoxicillin/clavulanate potassium combined with short-term low-dose dexamethasone in the treatment of children with suppurative tonsillitis.Methods80children with pediatric sup⁃purative tonsillitis treated in the hospital from January2016to January2018were randomly selected and enrolled in the study.They were randomly divided into control group and observation group.The patients were treated with anti-infective and symptomatic supportive treatment with amoxicillin and clavulanate potassium.The observation group was treated with low-dose dexamethasone for a short period of time.The clinical efficacy and medication safety of the two groups were com⁃pared.Results The general improvement time of the observation group was(2.12±0.18)d,the disappearance time of the ab⁃scess was(2.02±0.8)d,and the fever time was(2.07±0.59)d,which was significantly lower than the control group(t=5.273, 4.386,4.012,P<0.05);the total effective rate of treatment in the observation group was97.50%,which was significantly higher than that in the control group(χ2=18.131,P<0.05).There were no adverse reactions in the two groups.Conclusion The short-term use of low-dose dexamethasone for the treatment of pediatric suppurative tonsillitis based on amoxicillin clavulanate potassium has a more significant therapeutic effect and high safety,which is worthy of clinical reference.[Key words]Amoxicillin/Clavulanate potassium;Dexamethasone;Pediatric suppurative tonsillitis;Effect;Safety[作者简介]王莉(1975-),女,江苏如皋人,本科,主治医师,研究方向:小儿内科。
地塞米松抑制试验在亚临床库欣综合征诊断中的价值摘要】目的:分析地塞米松抑制试验在亚临床库欣综合征诊断中的价值。
方法:选取肾上腺意外瘤患者60 例,按照小剂量(2mg) 和大剂量(8mg)DST 分为三组,甲、乙、丙均为20 例。
甲组2mg 和(8mg)DST 均不能抑制;乙组(2mg)DST 不能抑制,(8mg)DST 能抑制;丙组中2mg 和(8mg)DST 均能抑制。
结果:本次研究中,其中有16 例大小剂量一致,15 例大小剂量不一致。
讨论:小剂量DST 对亚临床库欣综合征的诊断价值高。
【关键词】地塞米松;抑制试验;价值;亚临床库欣综合征【中图分类号】R2 【文献标号】 A 【文章编号】 2095-9753(2015)08-0068-02Dexamethasone suppression test in the diagnosis of subclinical Cushing's syndromeWu Fangfang (shangqiu first people's hospital endocrine laboratory Henan shangqiu, 476100)【 abstract 】 objective: to analysis dexamethasone suppression test value in the diagnosis of subclinical Cushing's syndrome.Selection methods: 60 patients with adrenal accidental tumors, according to the small dose (2 mg) and high dose (8 mg) DST was dividedinto three groups, a, b, c are in 20 cases. First division 2 mg and 8 mg (DST) can't restrain; (2 mg) DST can't restrain b, 8 mg (DST) canrestrain; 2 mg in c group and 8 mg (DST) can inhibit. Results: in this study, including 16 cases of size dose, 15 cases of size dose notconsistent. Discussion: a small dose of DST high value to the diagnosis of subclinical Cushing's syndrome.【 key words 】 : dexamethasone; Inhibition test; Value; Subclinical Cushing's syndrome在肾上腺意外瘤中,亚临床库欣综合征是最为常见的亚型,患者的临床表现症状是伴有代谢综合征,给患者的心血管系统带来极大的危害,为此,一定要及早发现,及早治疗。
The Low-Dose Dexamethasone Suppression Test:A Reevaluation in Patients with Cushing’s SyndromeJAMES W.FINDLING,HERSHEL RAFF,ANDDAVID C.ARONThe Endocrine-Diabetes Center (J.W.F.,H.R.),St.Luke’s Medical Center and Medical College of Wisconsin,Milwaukee,Wisconsin 53215;and Division of Clinical and Molecular Endocrinology,Department of Medicine (D.C.A.),Louis Stokes Department of Veterans Affairs Medical Center and Case Western Reserve University School of Medicine,Cleveland,Ohio 44106Low-dose dexamethasone suppression testing has been rec-ommended for biochemical screening when Cushing’s syn-drome is suspected.The criterion for normal suppression of cortisol after dexamethasone is controversial.To assess diag-nostic utility (sensitivity),we report the results of low-dose dexamethasone suppression testing in 103patients with spon-taneous Cushing’s syndrome.There were 80patients with Cushing’s disease (78%),13with the ectopic ACTH syndrome (13%),and 10with cortisol-producing adrenocortical adeno-mas (10%).Fourteen (18%)of 80patients with Cushing’s dis-ease suppressed serum cortisol to less than 5g/dl (<135nmol/liter)after the overnight 1-mg test,whereas six patients (8%)actually showed suppression of serum cortisol to less than 2g/dl (<54nmol/liter).In addition,the 2-d,low-dose dexameth-asone suppression test yielded false-negative results in 38%of patients when urine cortisol was used and 28%when urinary 17-hydroxycorticosteroids were used.Serum cortisol after the 1-mg test correlated with baseline urinary free cortisol (r ؍0.705,P <0.001),plasma ACTH level (r ؍0.322,P ؍0.001),and urinary free cortisol after the 2-d test (r ؍0.709,P ؍0.001).This study provides evidence that low-dose dexamethasone may suppress either plasma cortisol or urinary steroids to levels previously thought to exclude Cushing’s syndrome and that these tests should not be used as the sole criterion to exclude the diagnosis of endogenous hypercortisolism.(J Clin Endocrinol Metab 89:1222–1226,2004)THE DIAGNOSIS OF spontaneous Cushing’s syndrome is a very challenging problem in clinical endocrinology (1).The differentiation of patients with true pathological endogenous hypercortisolism from the large number of pa-tients with the Cushing’s phenotype may be very difficult.There are remarkable similarities between the metabolic syn-drome and Cushing’s syndrome.Excessive and sustained cortisol secretion has long been associated with the entire clinical spectrum of the metabolic syndrome including obe-sity,insulin resistance,dyslipidemia,hypertension,and di-abetes (1,2).Clinical improvement (e.g.blood pressure re-duction,weight reduction,and improvement in glycemic control)has been observed after adrenal surgery in some patients with incidentally discovered adrenocortical tumors and subclinical hypercortisolism.These observations em-phasize the importance of discovering and treating even mild Cushing’s syndrome (2–4).Biochemical confirmation of Cushing’s syndrome has re-lied upon the measurement of urinary free cortisol over a 24-h period and low-dose dexamethasone suppression test-ing (1).Low-dose dexamethasone suppression testing,espe-cially the 1-mg overnight test,has been the mainstay of biochemical screening and is recommended in most standard texts.Although it has been appreciated for many years that false-positive results are not uncommon with low-dose dexa-methasone suppression testing,it has previously been thought that false-negative results were relatively rare (1).There are three major concerns about applying publishedresults in clinical practice.First,the methodology of cortisol assays has changed over time,with newer assays having higher specificity (1,5).Second,the number of patients with Cushing’s syndrome in most series is relatively small.Consequently,the recommendations regarding low-dose dexamethasone sup-pression testing has been based on compilations of studies using different cut points,different protocols,and different methods of cortisol measurement (6).Finally,recommenda-tions have not sufficiently taken into account the distinction between efficacy and effectiveness (7).As applied to diagnostic testing,efficacy refers to the degree to which the test has been shown scientifically under ideal conditions to accomplish the desired outcome.In contrast,effectiveness refers to the degree to which the test achieves this outcome in actual clinical prac-tice.Most published studies have been performed in research venues using the same intramural assays and methodologies,and thus,are efficacy studies.On the other hand,the effective-ness of tests in clinical practice using a variety of approaches and reference laboratories has not been extensively evaluated.We studied 203consecutive patients with Cushing’s syn-drome referred to a single endocrinologist over a 15-yr pe-riod.To assess the effectiveness of low-dose dexamethasone suppression testing as a screening test,we now report the results from 103of these 203patients who had completed such testing.This study,performed in clinical practice,shows that some patients with Cushing’s syndrome suppress either plasma cortisol or urinary steroids to levels previously thought to exclude the diagnosis.Patients and MethodsStudy design and populationWe evaluated a case series of 203consecutive patients with Cushing’s syndrome referred to a single clinician (J.W.F.)from 1984–1998,of whomAbbreviation:17OH-corticosteroid,17-Hydroxycorticosteroids.JCEM is published monthly by The Endocrine Society (),the foremost professional society serving the en-docrine community.0021-972X/04/$15.00/0The Journal of Clinical Endocrinology &Metabolism 89(3):1222–1226Printed in U.S.A.Copyright ©2004by The Endocrine Societydoi:10.1210/jc.2003-0302071222103had completed low-dose dexamethasone suppression testing and were used for analysis of effectiveness.The diagnosis of spontaneous Cushing ’s syndrome was established in almost all patients by the re-ferring endocrinologist.The diagnosis of endogenous hypercortisolism was based on clinical findings and elevations of urinary free cortisol.Many other patients were referred with possible Cushing ’s syndrome,and the diagnosis was excluded.However,because these results were not available for analysis,our study is limited to the issue of test sensitivity.Biochemical testingMost biochemical test results were provided by the referring physi-cian(s).Measurement of both plasma cortisol and urine free cortisol used a variety of methods.Low-dose dexamethasone suppression testing was performed by the referring physician or by the consultant as follows.Either 1mg of dexamethasone was given at 2300h with serum cortisol measured the following morning or 0.5mg of dexamethasone was given every 6h for 48h,with measurement of urine free cortisol and/or 17-hydroxycorticosteroids (17OH-corticosteroids).One patient under-went the overnight 1-mg dexamethasone suppression test three times,and all three results were included in the analyses to avoid bias.Statistical analysisContinuous variables were compared using the nonparametric Mann-Whitney U test.Frequencies were analyzed by the Pearson 2test.Statistical analyses were performed using SPSS 11.0(SPSS,Chicago,IL).A P Ͻ0.05is reported as statistically significant.ResultsPatient characteristicsThe clinical characteristics of the 103patients who under-went dexamethasone testing did not differ from the 100patients who did not in terms of etiology of Cushing ’s syn-drome,duration of disease,prevalence of hypokalemia,andbasal values of urinary free cortisol and ACTH.The 103patients who underwent dexamethasone testing were slightly older;the median age was 44yr (range,10–78yr)in the tested group vs.40yr (range,11–79yr)in the group that was not tested (P ϭ0.035).We report detailed results of the 103patients with dexamethasone testing,of which 71were women (69%).There were 80cases of Cushing ’s disease (78%),13cases of the ectopic ACTH syndrome (13%),and 10cases of adrenal tumors (10%).Median baseline data were urinary free cortisol of 211g/24h [range,47–10,460g/24h (median,570nmol/24h;range,127–28,240nmol/24h)]and plasma ACTH of 57pg/ml [range,1–649pg/ml (me-dian,13pmol/liter;range,4–144pmol/liter)].Among the patients with a pituitary etiology (Cushing ’s disease),the median plasma ACTH was 58pg/ml [range,6–210pg/ml (median,13pmol/liter;range,1.3–47pmol/liter)].Test characteristics of low-dose dexamethasone suppression testingFigure 1shows that,in patients with Cushing ’s disease,six had serum cortisol of 2g/dl or less (Ͻ54nmol/liter),and eight had serum cortisol of 2–5g/dl (54–135nmol/liter),yielding false-negative rates of 7.5%and 17.5%,respectively.Patients with Cushing ’s disease whose postdexamethasone cortisol levels were 2g/dl or less (Ͻ54nmol/liter)had baseline urine-free cortisols of 51–275g/24h (138–742nmol/24h).Among the patients with adrenal tumors,the postdexamethasone cortisol levels ranged from 9.0–30.0g/dl (240–800nmol/liter).One patient underwent low-dose dexamethasone testing three times,with morningse-F IG .1.Distribution of plasma cortisol levels after 1mg dexamethasone given at 2300h in patients with Cushing ’s disease (n ϭ82data points).To convert to nmol/liter,multiply morning cortisol by 27.6.Therefore,the scale of plasma cortisol is Ͻ55to Ͼ276nmol/liter.Findling et al.•Dexamethasone Testing in Cushing ’s Syndrome J Clin Endocrinol Metab,March 2004,89(3):1222–12261223rum cortisol values of3,6,and12g/dl(81,162,and324 nmol/liter).Because two of three of these results were true positives(Ͼ5g/dl),we included all three in the analysis to be conservative.Characteristics of patients with Cushing’s disease whose postdexamethasone cortisol was2g/dl or less(Ͻ54nmol/ liter)are shown in Table1.Of these six patients with Cush-ing’s disease,two patients had proven ACTH-secreting pituitary microadenomas.The remaining four patients did not have histologically proven ACTH-secreting tumors.Of these,three patients actually had intermittent elevations of urinary cortisol,and the dexamethasone suppression testing may have been performed when the patient was eucorti-solemic.Nonetheless,of the four patients without histolog-ically proven corticotroph adenomas,one patient had tran-sient secondary adrenal insufficiency followed by clinical and biochemical remission after hemihypophysectomy.Two of the patients developed eucortisolemia after partial hy-pophysectomy but did not develop secondary adrenal in-sufficiency,and one patient had permanent hypoadrenalism after hypophysectomy.It is possible that the hypercorti-solism in these other three patients was not due to pathologic Cushing’s syndrome.Furthermore,the eight patients with postdexamethasone cortisol levels of2–5g/dl(54–135 nmol/liter)had surgically confirmed ACTH-secreting pitu-itary adenomas.We next examined the results of2-d,low-dose dexameth-asone suppression tests.This test was performed in a total of 59patients;the urinary-free cortisol responses were assessed in54patients,and the17OH-corticosteroid responses were assessed in30patients.The postdexamethasone values for urinary free cortisol ranged from undetectable to3286g/24 h(8850nmol/d);the17OH-corticosteroid values ranged from undetectable to102mg/24h(282mol/d).Nine pa-tients had urinary free cortisol that suppressed to less than 10g/24h(Ͻ27nmol/24h;16.7%false negative).Two patients had urinary17OH-corticosteroid levels that sup-pressed to less than2.5mg/d(Ͻ6.9mol/d;6.7%false negative),and five patients had levels that suppressed to3 mg/24h or less(Յ8mol/d;16.7%false negative). Serum cortisol after the1-mg test correlated with the base-line urinary free cortisol(rϭ0.705,PϽ0.001),plasma ACTH level(rϭ0.322,Pϭ0.001),and urinary-free cortisol after the 2-d test(rϭ0.709,Pϭ0.001),but it did not correlate with urinary17OH-corticosteroids after the2-d test(rϭ0.038,Pϭ0.91).Because there were some extremely elevated levels of urinary free cortisol among patients with ectopic ACTH syn-drome and adrenal tumors,we assessed the relationship between cortisol and other tests in the patients with Cush-ing’s disease(Fig.2).In this subgroup of patients with Cush-ing’s disease,serum cortisol after the1-mg test correlated with the baseline urinary free cortisol(rϭ0.535,PϽ0.001), urinary-free cortisol(rϭ0.730,Pϭ0.001),and urinary 17OH-corticosteroids(rϭ0.800,Pϭ0.005)after the2-d test. However,there was no significant correlation with plasma ACTH(rϭ0.058,Pϭ0.612).DiscussionThis study provides evidence that neither the overnight 1-mg dexamethasone suppression test nor the2-d,low-dose dexamethasone suppression test should be used as the sole criterion to exclude the diagnosis of Cushing’s syndrome. Previous studies have shown the sensitivity of low-dose dexamethasone suppression testing,particularly the over-night1-mg dexamethasone test,to range from83–100%(5,6, 8–15).These studies have differed in the type of cortisol assays used,the doses of dexamethasone employed,and the criteria for a positive test.A recent survey of laboratories in the United Kingdom in-dicated that the majority of pathologists recommended the overnight low-dose dexamethasone suppression test as a screening procedure for patients with suspected Cushing’s syn-drome(16,17).Among127laboratories,91used a dose of1mg, three used a dose of1.5mg,and33used a dose of2mg. Reported cutoff values for the suppression of serum cortisol in other studies using contemporary immunoassay techniques range from3.6–7.2g/dl(70–100nmol/liter).These patholo-gists suggested that dexamethasone-induced suppression of plasma cortisol to less than1.8g/dl(Ͻ50nmol/liter)effec-tively excluded Cushing’s syndrome.The application of this stringent cutoff to safely exclude Cushing’s syndrome was also endorsed recently at an international workshop on the diag-nosis,complications,and treatment of Cushing’s syndrome (18).As our study demonstrates,some patients with mild Cush-ing’s disease demonstrated marked sensitivity to dexametha-sone suppression;therefore,a much lower cutoff value than has been previously used in clinical practice should be used to achieve adequate sensitivity.However,our data from clinical practice patterns in the United States provide evidence that there is no cutoff value that achieved100%sensitivity.More-over,as the cutoff value is lowered to increase the sensitivity,TABLE1.Characteristics of patients with Cushing’s disease and postdexamethasone cortisol levels2g/dl or lessCase no.Age(yr)Baseline UFC[g/d(nmol/d)]Other findings Pathology 138202(558)Abnormal dexamethasone-CRH test ACTH pituitary tumor278128(353)Abnormal dexamethasone-CRH test ACTH pituitary tumor33697(268)Intermittent Cushing’s Hemihypophysectomy resulted insecondary adrenal insufficiencyand clinical remission 440275(759)Abnormal dexamethasone-CRH test Hypophysectomy;no tumor541274(756)Intermittent Cushing’s Hemihypophysectomy resulted inbiochemical remission 62751(141)Intermittent Cushing’s Hemihypophysectomy resulted inbiochemical remissionUFC,Urinary free cortisol.1224J Clin Endocrinol Metab,March2004,89(3):1222–1226Findling et al.•Dexamethasone Testing in Cushing’s Syndromethe false-positive rate for the low-dose dexamethasone sup-pression test will inevitably increase significantly,thereby de-creasing the overall diagnostic utility of this test.Gorges et al.(9)studied 247patients with suspected Cush-ing ’s syndrome,of whom 103patients had the disorder.They found that the 1.5-mg overnight dexamethasone suppression test had a sensitivity of 98%and 94%using cutoffs of 2.6g/dl (70nmol/liter)and 5.2g/dl (140nmol/liter),re-spectively.The lowest plasma cortisol achieved after the low-dose test in a patient with proven Cushing ’s syndrome was 1.2g/dl (32nmol/liter).Some investigators have dem-onstrated that the measurement of serum cortisol (rather than urinary steroids)after the 2-d,low-dose dexamethasone suppression testing provides improved sensitivity and spec-ificity.Newell-Price et al.(19)reported that a serum cortisol of less than 1.8g/dl (50nmol/liter)after the administration of 0.5mg dexamethasone every 6h for 48h resulted in a sensitivity of 98%.They also found that only three of 150patients with histologically proven Cushing ’s disease sup-pressed to less than 1.8g/dl (50nmol/liter)(19).Invitti et al.(20)reported another large series using criteria for sup-pression of serum cortisol to less than 5g/dl (135nmol/liter)after the overnight 1-mg dexamethasone suppression test as well as suppression of urine free cortisol and 17OH-corticosteroids less than 20g/24h (55nmol/d)and 3.5mg/24h (7mol/d),respectively,after 0.5mg of dexameth-asone every 6h for 2d.They found the sensitivity to be 95%for the overnight test and 93%for the 2-d test.Their total series consisted of 426patients,in whom 104had adrenal-dependent Cushing ’s syndrome.Because the sensitivity of dexamethasone suppression testing in patients with adrenal tumors is higher than in other causes of Cushing ’s syndrome,the high prevalence of adrenal-dependent hypercortisolism in their series biased the results in such a way as to put the dexamethasone test in an even more favorable light.The National Institutes of Health group evaluated theclassic 2-d,low-dose dexamethasone suppression test in a large series of patients with mild Cushing ’s syndrome and compared them to patients with pseudo-Cushing ’s condi-tions (21).The classic 2-d,low-dose dexamethasone suppres-sion test yielded a sensitivity of only 79%,a specificity of 74%,and a diagnostic accuracy of 71%using urinary steroid mea-surements.Our study showed that 14(17%)of 80patients with Cushing ’s disease suppressed serum cortisol to less than 5g/dl (Ͻ135nmol/liter)after the overnight 1-mg test.In addition,six patients actually showed suppression of se-rum cortisol to less than 2g/dl (Ͻ54nmol/liter)with the overnight test.The 2-d,low-dose dexamethasone suppres-sion test yielded false-negative results in 38%of our patients when urine free cortisol was used and 28%of our patients when urinary 17OH-corticosteroids were used.The results of our study are also similar to those reported by Streeten et al.(22),who showed that,in 58patients with proven Cushing ’s disease,23%had suppression of urine free cortisol to very low levels after the low-dose dexamethasone suppression test.There was remarkable and significant correlation of basal urine free cortisol and the plasma cortisol after the low-dose dexamethasone suppression test in our patients with Cushing ’s disease.In other words,patients with mild degrees of hyper-cortisolism were more likely to suppress their plasma cortisol to low levels after the overnight 1-mg dexamethasone suppres-sion test.All eight patients with Cushing ’s disease whose cor-tisol level decreased to 2–5g/dl (54–135nmol/liter)had sur-gically proven ACTH-secreting microadenoma.Of the six patients with Cushing ’s disease who had cortisol values of less than 2g/dl (Ͻ54nmol/liter)after the over-night test,three patients did not have either ACTH-secreting pituitary microadenomas or evidence of secondary adrenal insufficiency after hemihypophysectomy.Although the hy-percortisolism remitted in the other three patients after sur-gery,it is possible that the cortisol excess in these patients may not have been due to pathological Cushing ’s syndrome.The intermittent nature of hypercortisolism in two of these patients would also confound the postoperative biochemical evaluation.Consequently,this observational data suggests that the sensitivity of the overnight 1-mg dexamethasone suppres-sion test in the diagnosis of Cushing ’s disease is somewhere between 93–96%when a strict criteria of less than 2g/dl (Ͻ54nmol/liter)is used as normal cortisol suppression.We studied the sensitivity of low-dose dexamethasone suppression testing for the diagnosis of Cushing ’s syndrome.Our analysis relied upon the results of dexamethasone sup-pression testing supplied by referring clinicians.This means that a variety of clinical laboratories and methods were used to measure plasma and urinary steroids.This approach is not likely to provide the precision found in efficacy studies per-formed in a clinical research center using a single method-ology and batch assays.Similarly,it is not likely that dexa-methasone suppression testing in a real-world setting can match that achieved in the research setting.Therefore,our data are more representative of the results likely to be ob-tained by practicing physicians.A limitation of this study is a possibility of selection bias,especially because disease prevalence is important in gen-eralizing clinical prediction rules.Ideally,evaluation of dexa-methasone suppression testing should be performed onaF IG .2.Correlation between serum cortisol after overnight dexa-methasone suppression and baseline urinary free cortisol in patients with Cushing ’s disease (r ϭ0.52,P Ͻ0.001,n ϭ82data points).To convert urine free cortisol to nmol/liter,multiply by 2.76.Therefore,the scale of urine free cortisol is 28–27,600nmol/d.To convert morn-ing cortisol (serum)to nmol/liter,multiply by 27.6.Therefore,the scale of morning cortisol is 0–1656nmol/liter.Findling et al.•Dexamethasone Testing in Cushing ’s Syndrome J Clin Endocrinol Metab,March 2004,89(3):1222–12261225population-based rather than a referral-based sample.Spon-taneous Cushing’s syndrome is an unusual disorder.Con-sequently,all large series of patients reflect referral patterns. Bias may result from the referral of difficult cases for spe-cialized expertise,such as inferior petrosal sinus sampling. Such difficult cases may be those with atypical laboratory results.Nonetheless,our observations strongly suggest that the sensitivity for low-dose dexamethasone suppression test-ing for the diagnosis of Cushing’s syndrome has been over-estimated.The problem of intermittent hypercortisolism in some patients with Cushing’s syndrome provides further diagnostic uncertainty in the evaluation of this enigmatic disorder(23).We certainly acknowledge that some of these false-negative,low-dose dexamethasone suppression results may be due to this intermittency.The interval time between the low-dose dexamethasone test and urine cortisol may also account for some of this discordance.The phenomenon of intermittent or periodic hypercortisolism potentially con-founds any diagnostic study for Cushing’s syndrome.We currently use repeated measurements of late-night salivary cortisol to confirm the presence or absence of intermittent hypercortisolism(24–26).We conclude that some patients with spontaneous Cush-ing’s syndrome,particularly those with mild hypercorti-solism,may suppress plasma or urinary steroids after low-dose dexamethasone to levels previously thought to exclude the diagnosis.Therefore,low-dose dexamethasone tests should not be used alone to exclude the diagnosis of Cush-ing’s syndrome,and a much lower value for serum cortisol (i.e.Ͻ1.8g/dl;Ͻ50nmol/liter)should be used to achieve adequate sensitivity.AcknowledgmentsThe authors thank Drs.Joseph Shaker,Steven Magill,and Beth La-lande for their invaluable contributions to this study.Received February10,2003.Accepted November24,2003.Address all correspondence and requests for reprints to:James W. Findling,M.D.,St.Luke’s Physician’s Office Building,Endocrinology, Suite245,2801W.Kinnickinnic River Parkway,Milwaukee,Wisconsin 53215-3660.E-mail:james.findling@.References1.Findling JW,Raff H2001Diagnosis and differential diagnosis of Cushing’ssyndrome.Endocrinol Metab Clin North Am30:729–7472.Terzolo M,Pia A,Ali A,Osella G,Reimondo G,Bovio S,Daffara F,ProcopioM,Paccotti P,Borretta G,Angeli A2002Adrenal incidentaloma:a new cause of the metabolic syndrome?J Clin Endocrinol Metab87:998–10033.Agency for Healthcare Research and Quality2002Evidence report/technol-ogy assessment number56:management of clinically inapparent adrenal mass.Agency for Healthcare Research and Quality Publication No.02-E014;Rock-ville,MD;4.Tauchmanova L,Rossi R,Biondi B,Pulcrano M,Nuzzo V,Palmieri E-A,Fazio S,Lombardi G2002Patients with subclinical Cushing’s syndrome dueto adrenal adenoma have increased cardiovascular risk.J Clin Endocrinol Metab87:4872–48785.Ritchie JC,Carroll BJ,Olton PR,Shively V,Feinberg M1985Plasma cortisoldetermination for the dexamethasone suppression test:comparison of com-petitive protein-binding and commercial radioimmunoassay methods.Arch Gen Psychiatry42:493–4976.Crapo L1979Cushing’s syndrome:a review of diagnostic tests.Metabolism9:955–9777.Aron DC,Raff H,Findling JW1997Effectiveness versus efficacy:the limitedvalue in clinical practice of high dose dexamethasone suppression testing in the differential diagnosis of adrenocorticotropin-dependent Cushing’s syn-drome.J Clin Endocrinol Metab82:1780–17858.Kaye TB,Crapo L1990The Cushing syndrome:an update on diagnostic tests.Ann Intern Med112:434–4449.Gorges R,Knappe G,Gerl H,Ventz M,Stahl F1999Diagnosis of Cushing’ssyndrome:re-evaluation of midnight plasma cortisol vs urinary free cortisol and low-dose dexamethasone suppression test in a large patient group.J Endocrinol Invest22:241–24910.Holdaway IM,Evans MC,Ibertson HK1973Experience with a short test ofpituitary-adrenal function.Aust N Z J Med3:507–51111.Asfeldt VH1969Simplified dexamethasone suppression test.Acta Endocri-nologica61:219–23112.Nugent CA,Nichols T,Tyler FH1965Diagnosis of Cushing’s syndrome.Single dose dexamethasone suppression test.Arch Intern Med116:172–176 13.Pavlatos FC,Smilo RP,Forsham PH1965A rapid screening test for Cushing’ssyndrome.JAMA193:96–9914.Tucci JR,Jagger PI,Lauler DP,Thorn GW1967Rapid dexamethasone sup-pression test for Cushing’s syndrome.JAMA199:129–13215.Barrou Z,Guiban D,Maroufi A,Fournier C,Dugue M-A,Luton J-P,Tho-mopoulos P1996Overnight dexamethasone suppression test:comparison of plasma and salivary cortisol measurement for the screening of Cushing’s syndrome.Eur J Endocrinol134:93–9616.Barth J,Seth J,Howlett TA,Freedman DB1995A survey of endocrinefunction testing by clinical biochemistry laboratories in the UK.Ann Clin Biochem32:442–44917.Wood PJ,Barth JH,Freedman DB,Perry L,Sheridan B1997Evidence for thelow dose dexamethasone suppression test to screen for Cushing’s syndrome—recommendations for a protocol for biochemistry laboratories.Ann Clin Bio-chem34:222–22918.Arnaldi G,Angeli A,Atkinson AB,Bertagna X,Cavagnini F,Chrousos G,Fava GA,Findling J,Gaillard RC,Grossman AB,Kola B,Lacroix A,Mancini T,Mantero F,Newell-Price J,Nieman LK,Sonino N,Vance ML,Giustina A, Boscaro M2003Diagnosis and complications of Cushing’s syndrome:a con-sensus statement.J Clin Endocrinol Metab88:5593–560119.Newell-Price J,Trainer P,Perra L,Wass J,Grossman A,Besser M1995Asingle sleeping midnight cortisol has100%sensitivity for the diagnosis of Cushing’s syndrome.Clin Endocrinol(Oxf)43:545–55020.Invitti C,Giraldi FP,De Martin M,Cavagnini F1999Diagnosis and man-agement of Cushing’s syndrome:results of an Italian multicentre study.J Clin Endocrinol Metab84:440–44821.Yanovski JA,Cutler Jr GB,Chrousos GP,Nieman LK1993Corticotropin-releasing hormone stimulation following low-dose dexamethasone adminis-tration.A new test to distinguish Cushing’s syndrome from pseudo-Cushing’s states.JAMA269:2232–223822.Streeten DHP,Anderson CH,Brennan S,Jones C1998Suppressibility ofplasma adrenocorticotropin by hydrocortisone:potential usefulness in the diagnosis of Cushing’s disease.J Clin Endocrinol Metab1114–112023.Hermus AR,Pieters GF,Borm GF,Verhofstad AA,Smals AG,Benraad TJ,Kloppenborg PW1993Unpredictable hypersecretion of cortisol in Cushing’s disease:detection by daily salivary cortisol measurements.Acta Endocrinol 128:428–43224.Raff H,Raff JL,Findling JW1998Late-night salivary cortisol as a screeningtest for Cushing’s syndrome.J Clin Endocrinol Metab83:2681–268625.Papanicolaou DA,Mullen N,Kyrou I,Nieman LK2002Nighttime salivarycortisol:a useful test for the diagnosis of Cushing’s syndrome.J Clin Endo-crinol Metab87:4515–452126.Raff H,Findling JW2003A physiologic approach to the diagnosis of Cush-ing’s syndrome.Ann Intern Med138:980–991JCEM is published monthly by The Endocrine Society(),the foremost professional society serving theendocrine community.1226J Clin Endocrinol Metab,March2004,89(3):1222–1226Findling et al.•Dexamethasone Testing in Cushing’s Syndrome。